For you who have undergone surgery for a fractured wrist
There are two bones in the forearm – the radius and the ulna.
A radius fracture is one of the most common fractures. All fractures are different, depending upon the appearance of the injury and the nature of the accident. Therefore, you can’t compare your injury with your friend’s broken wrist. The diagnosis is confirmed using an X-ray. There are different fixation methods for radius fractures.
The method is determined according to the appearance of the fracture;
- Surgery with a fixation plate or pins, may be used in combination with a cast
- Hoffman (external fixator)
- Cast only
Plate
A surgical procedure that is used frequently to stabilize the fracture, is the use of a metal plate that is attached to the bone, underneath the soft tissue and skin. The scar will normally be on the inside of the wrist.
The metal plate, which is small and thin, fixates the fracture using screws that are placed on either side of the fracture. The metal plate is normally made of titanium, although other metals may be used,
depending on the type of plate.
After surgery you will normally wear a cast for 2 weeks. This will be removed at the same time as the stitches are removed. However, depending on the physician’s assessment, you might need to wear the cast for a shorter or longer period. If your fracture is stabilized by using a cast, it is important that the cast doesn’t get wet as this will weaken it. When showering, use a plastic bag to cover the cast and seal it with surgical tape.
After surgery, the stitches will normally be removed after 2 weeks. Don’t wash the wound during the first 2-3 days (pins 4-5 days). It is a good idea to have surgical tape on the wound/scar as protection.
The amount of weight you can put on your hand during healing is limited during the first 6-8 weeks after surgery. During this period, you shouldn’t carry or lift heavy objects. You should also avoid the pulling open or pushing heavier doors etc. The amount of weight you can put on your hand is determined by the surgeon.
When the cast is removed it is normal to have some stiffness in the movement of your wrist and forearm. The strength of your hand will be reduced, and you might experience pain. This is partly due to the operation and having a cast, but mainly due to the injury to the soft tissues (ligaments, tendons and muscles) that occurred at the time of your fracture.
Exercising the wrist should start as soon as the cast has been removed.
The plate is quite often left in place after healing is complete but may be surgically removed if it causes problems. Continued pain or discomfort often depends on the soft tissues and not the plate.
Hoffmaninstrument
Using a Hoffman means that the fracture is fixed using a frame on the outside of the skin, a so-called external fixation or Hoffman.
Two threaded pins are screwed into the radius bone above the fracture, and two threaded pins are screwed into the hand. The two pairs of threaded pins are connected to a metal rod. The Hoffman is normally attached for four to six weeks.
It is important that you, keep the skin around the pins dry for approx. 10 days after the surgery. Use a plastic bag and surgical tape on your arm when having a shower.
To avoid an infection around the pins, it is important that the instructions below are followed, after the 10-day control at the orthopedic department:
Daily
- Rinse the skin and frame with lukewarm water in the shower
- Wash the skin around the pins with liquid soap and water
The scab around the pins and wound edge can be removed with a clean toothbrush or cotton swab. Rinse in the shower and dry with a clean towel. Let the skin air dry afterwards
Generally
- Don’t use alcohol or iodine solutions
- Avoid using thick dressings, creams and impregnated dressings Having clean and dry skin round the pins is the best protection against infections
Pins
An alternative method to fixate the fracture is to insert metal pins to hold the bones in the correct position while they heal. The wrist is also placed in a cast, usually for about 4 weeks. If your fracture is stabilized by using a cast, it is important that the cast doesn’t get wet as this will weaken it.
Generally
Contact the Orthopedic Department in the following cases:
- Increased or new pain in or around the fracture
- Fever (which is not due to another illness)
- The cast is pressing or rubbing on your skin
- Your fingers are very swollen or shiny (you can also contact the Hand Therapist)
- Numbness
- Severe pain or coldness
- Pus in the wound around the pins (Hoffman)
- The construction of the frame feels loose or unstable (Hoffman)
- Redness or swelling of the skin around the pins (Hoffman)
- If you feel unsure or have any questions
Advice during time of fixation
- When using your arm, keep it as relaxed and use it as naturally as possible
- Use your arm when doing lighter everyday tasks
- Rest your arm in an elevated position above your heart when you’re not using it
- Avoid heavy carrying and heavy lifting
- Only wear a sling for your arm if it has been prescribed
Pain
Make sure you take the prescribed painkillers as soon as the anesthesia wears off after the operation. It is normal to feel pain for the first couple of weeks, and you may need to take painkillers regularly, particularly during the day. To feel pain in the shoulder is also common after suffering an injured wrist. The pain will decrease when you start to move your shoulder more actively.
If you continue to have problems with your shoulder, please contact a physio therapist at your local GP or healthcare centre:
Call 1177 or contact us via 1177 e-services.
Call 0046 771-11 77 00 if your phone does not have a Swedish subscription or SIM card, or if you are calling from another country.
Swelling
A fractured wrist usually causes swelling of the hand. This is due to reduced mobility of the arm, and the muscles can’t work normally to help pump tissue fluid back into the blood stream. Reducing swelling is important as it helps to reduce pain and increase mobility. It is normal for the hand to feel swollen and stiff in the morning.
To avoid swelling it is important that you:
- When possible, use your hand to do everyday tasks
- Exercise by raising your arms in an upward stretch at the same time
- as you gently clench your fist and then spread your fingers. Do this approx. 10 times /hour during waking hours
- Avoid hot hand baths and saunas
- Avoid walking with your arm hanging down for a long period of time.
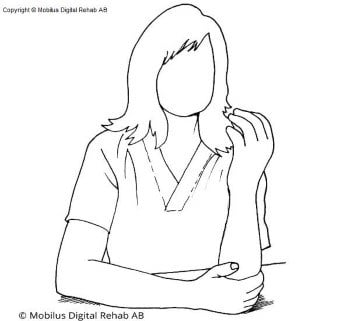
Using your hand in everyday life
The best training is to start using your hand as normally as possible. Try to use your hand for light tasks, such as combing your hair, eating, browsing through a magazine, washing up and personal hygiene.
It is important to let the injured hand be a part of all your everyday activities and not to let the “healthy” hand take over.
The first professor of hand surgery in Sweden, Erik Moberg, expressed it in the following way:
“The best way to train an injured hand is to put the healthy one in a cast”.
Exercise
It can be problematic with mobility after a fracture. The hand therapist will guide you through a suitable training program designed for your hand. The purpose of the exercises is to reduce the swelling and improve the mobility and strength in your hand. It is normal for it to hurt and feel tight when doing these exercises, but there is no risk of a new fracture occurring. Perform each movement slowly and remain focused. It is important to train actively with the injured hand, and not use the “healthy” hand for support.
Improvements in mobility and strength can occur up to a year after the injury. Your efforts during training are of great importance to the final result.
Exercise program during fixation
Even during the time when your hand is immobilized, it is important to exercise the joints that are not immobilized.
- Start exercising the day after you receive your cast
- Don’t use your other hand to increase the movement
- Stretch your hand as far as you can and hold it for about 5 seconds in this extended position
- Perform this program approx. 4 times/day, doing each exercise approx. 10 times, if no other instructions have been given.
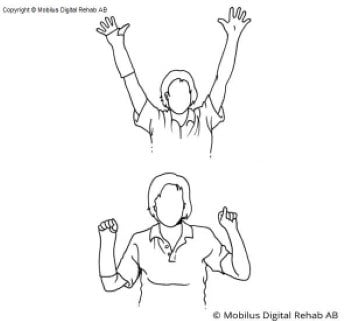
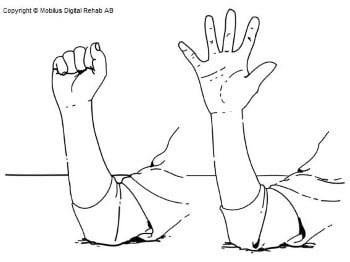
1.
- Raise and stretch your arms upwards, spread your fingers.
- Clench your fists and bring your arms down to the starting position.
Exercise arms in an upward stretch 10 times/hour during waking hours
2.
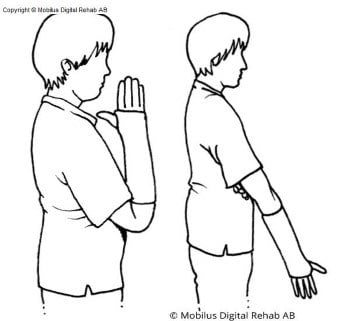
- Place the upper arm next to the body
- Bend and stretch the elbow.
3.
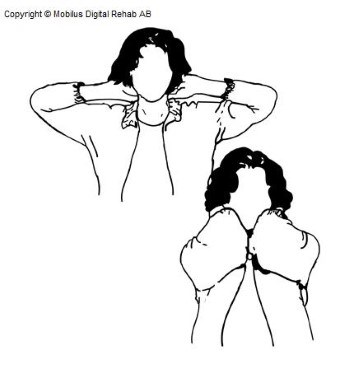
- Place both hands on either side of the head.
- Bring your elbows together in front of your face, then angle out
elbows to the sides again.
4.
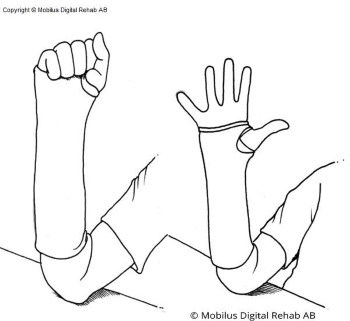
- Place the injured arm with the elbow on a table.
- Hold your thumb out.
- Clench your fingers all the way to the palm or cast.
- Stretch and spread properly with your fingers.
5.
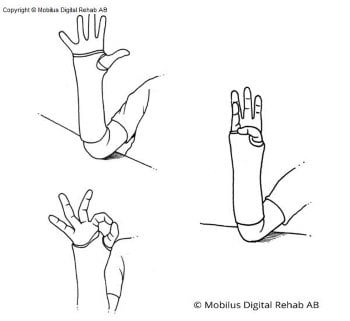
- Bring your thumb in a wide arch to the tip of the index finger,
stretching your thumb and fingers.
Continue in the same way for the middle finger, ring finger, little
finger and finally to the base of the little finger. - Important to extend both thumb and fingers between each
finger that the thumb meets.
Exercise program after the removal of the cast
- Perform this program approx. 4 times/day, doing each exercise approx. 10 times, if no other instructions have been given.
- Stretch your hand as far as you can and hold it for about 5 seconds in this extended position
- Start with exercise 1-3
1.
- Place the injured arm with the elbow on a table.
- Hold your thumb out.
- Clench your fingers all the way to the palm of your hand.
- Stretch and spread your fingers properly.
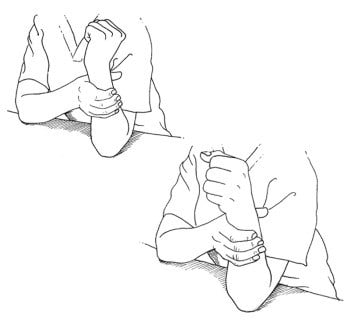
2.
- Place the elbow of the injured arm on a table.
- Arm in "arm-wrestler position".
- Rotate the palm toward you 10 times, returning to the arm-wrestler position between each rotation.
- Twist the palm away from you 10 times, returning to the arm-wrestler position between each twist.
3.
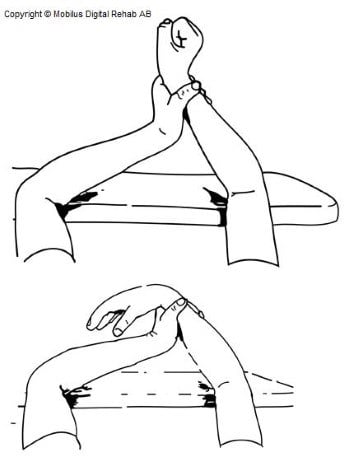
- Place the elbow of the injured arm on a table.
- Grip the injured arm in the middle of the forearm with the help of the healthy hand.
- Fold the injured arm in front of your body so you can watch
the wrist. - Clench your fingers gently and bend your wrist backwards and hold.
- Relax your fingers and angle your wrist forward.
4.
- Elbows on the table.
- Grip the injured arm.
- Move your wrist from side to side in an alternating motion, start
by moving it towards your little finger and then back toward
your thumb. - The movement is similar to how you angle your wrist when throwing an arrow.
If you have any questions regarding your injury or if you need to reschedule your appointment, please contact our reception + 46 8 123 553 22
Orthopedic Department
Callback service, phone: +46 8 123 569 12
Contact us if you need advice and support regarding your treatment, rescheduling of your appointment, getting help to book medical transport, cancelling your appointment or if you have any other questions regarding your referral. There are many people calling, so try to call earlier in the day to increase your chances of receiving a callback time.
You can also contact us via 1177 e-services.
Call 0046 771-11 77 00 if your phone does not have a Swedish subscription or SIM card, or if you are calling from another country.
Emergency department (ED)
Danderyds Hospital, switchboard:
phone 08-123 550 00